April 12, 2013, by Graham Kendall
What is Autism?
In this What is? series, we invite experienced researchers to write about their area of research, but in more general terms than they might normally do.
This article, entitled What is Autism?, is written by Prof. Peter Mitchell
If you would like to contribute, then please let me know (Graham.Kendall@nottingham.edu.my) and we can discuss how best to go about it.
Anybody wishing to contact the author of this article should go to about the author.
What is Autism?
Autism is a life-long developmental disorder and at present there is no known cure, though some affected individuals can adapt to their condition and function well in society with the right kind of learning experience. There are three distinctive and defining features of autism: (1) Impairment in social behaviour and relatedness to others; (2) Impairment in verbal and nonverbal communication; (3) Narrowing of interests coupled with resistance to change. Wing and Gould (1979) identified these features as the ‘triad of impairments’ that are the hallmark of autism. These are the features that a clinician looks for when deciding whether or not a diagnosis is warranted.
Just as the physiological basis of autism remains a mystery, so the causes are not fully understood. One possibility is that there are multiple causes. What matters might be damage to a particular site in the brain, rather than how that damage came about. Just as paralysis could be caused by injury, such as a fractured skull, stroke, or genetic abnormality where part of the brain fails to develop normally, so autism could have multiple causes. There is an important difference, however. Whereas paralysis could occur later in life, that would not be true of autism. An individual who has autism will have had it from the beginning. It seems that the brain abnormality responsible for autism prevents development in the spheres of social behaviour, communication and openness to having a variety of interests. Once those developments have already taken place, probably they cannot be reversed by brain abnormalities that are acquired later in life.
Prevalence and Historical details
Autism used to be regarded as a rare disorder, affecting fewer than 1 per thousand of the population, but rates of diagnosis have increased and it now seems that the incidence of autism (at least in its broadest form) stands at around 1 per hundred of the population (Baird et al, 2006). It is not entirely clear why rates of diagnosis are increasing, but a concomitant decrease in diagnosis of children with general learning disabilities suggests that clinicians are being more inclusive in diagnosing autism. Additionally, more children are being diagnosed who do not have accompanying learning disability. In previous years, suspected learning disability would have been the principal reason for clinical referral, whereas now, with growing awareness of autism, even children who do not have accompanying learning disability are likely to be referred if they present with severe social impairment.
Many more boys than girls tend to be diagnosed with autism and the ratio stands at 4:1. There is a broad spectrum of autism from mild to severe, where the mild forms include Asperger’s syndrome. This is diagnosed in individuals who have characteristically autistic social impairment but who have no accompanying language delay.
Autism Cartoon: Downloaded from Google (6 Apr 2013), labelled as free to reuse (Original image http://www.flickr.com/photos/57570482@N06/5299265960/)
Autism was first recognized as a disorder in its own right in the 1940s. It was identified independently by Leo Kanner working in the USA and Hans Asperger working in Austria. Both hit upon the name ‘autism’ to mean social detachment or social non-integration. The cases Kanner identified were rather severe, while Asperger identified individuals with both severe and mild forms of autism. Hence, those affected mildly tend to be diagnosed with Asperger’s syndrome. Just because autism has been defined fairly recently, it does not imply that it is a new disorder, like AIDS. Autism has probably been around pretty much forever, and biographies of maladapted children such as the Wild Boy of Aveyron in the Nineteenth Century are evidence for the existence of autism well before the label was used (Frith, 2003). Earlier in the Twentieth Century some with autism were diagnosed as having childhood schizophrenia. This label now seems wholly inappropriate when considering that core symptoms of schizophrenia, such as delusions, are thought not to occur prior to adolescence.
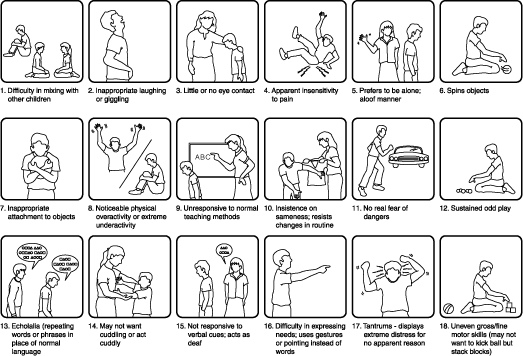
The leaflet published by the National Autistic Society for non-specialists and parents gives some idea of autism. It illustrates characteristic behaviours, and perhaps helps us to appreciate what autism is not. Autism is not an appropriate label for learning difficulties of a general nature. For example, it would be uncommon for a child with Down’s syndrome to receive a diagnosis of autism. A child with Down’s syndrome is very likely to have general learning difficulties but probably would not have the more specific kind of impairment that characterises autism. Autism, then, is a special kind of intellectual impairment.
What are the signs of autism?
Children with autism sometimes seem indifferent to others. Although they recognize people they know, they sometimes do not display more familiarity or affection towards them than to a complete a stranger. Their indifference is also manifest as lack of enthusiasm for playing with other children. They might join in with others if coaxed, but do not play as such. Generally, those with autism have a conspicuous impairment in social functioning and exhibit difficulties in verbal and nonverbal communication. The most severe form of disruption to verbal communication in autism is apparent in children who remain either permanently mute or who have extremely delayed language and communicative development. Children who do communicate verbally show various peculiarities in their speech. For example, some repeat what they hear as a kind of echo or parroting. Perhaps linked with that, they also show reversal of personal pronouns, where they sometimes address others as ‘I’ and refer to themselves as ‘you’.
Research into the social cognition of autism
Researchers have claimed that people with autism are handicapped by a specific impairment in interpreting psychological information from the region of the eyes (Baron-Cohen et al, 1997) and that specifically they have difficulty following gaze (Klin et al, 2002). However, research conducted at the University of Nottingham seriously challenges these claims. First, while high functioning adults with autism are not quite as good as comparison participants in guessing a person’s emotion from their facial expression, this is not because they are specifically impaired in interpreting information emanating from the region of the eyes (Back, Ropar & Mitchell, 2007).
Second, using various different kinds of methods, including eye movement recording technology, it has become abundantly clear that high functioning adults with autism can indeed follow the gaze of another person (Freeth et al, 2011). The essential difference between those with and without autism seems to be in the timing of their response. Freeth et al found that people with autism were about one second slower that typically developing participants to respond to a social cue like a shift in gaze direction. In contrast, though, participants with autism were faster in some cases to respond to physical stimuli compared with typically developing participants. The slowness to respond to social cues among people with autism might be a serious disadvantage in social encounters. During conversation, many fleeting social cues are emitted and humans are normally well adapted to keep pace with the rapid flow of information. Anyone who could not process social information at such speed would probably find that they were left behind and consequently excluded from the interpersonal intimacies and meeting of minds that most of us enjoy.
About the Author
Peter Mitchell is Dean of Science at the University of Nottingham Malaysia Campus, Previously, he served as the head of the School of Psychology in Nottingham UK (2005-2009). He has also worked at various other institutions including the University of Oxford, McGill University (Montreal), Warwick University and University of Birmingham. He has published seven books and more than 80 research articles in peer-review international journals and some of this work has been recognised with national prizes in the UK. He has served as Chair of the Developmental Section of the British Psychological Society and as Chief Examiner for the ESRC PhD Studentship Competition.
References
- Back, E. Ropar, D. & Mitchell, P. (2007). Do the eyes have it? Inferring mental states from animated faces in autism. Child Development, 78, 397-411.
- Baird, G., Simonoff, E., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., et al. (2006). Prevalence of disorders of the autism spectrum in a population cohort of children in south thames: The special needs and autism project (snap). Lancet, 368(9531), 210-215.
- Baron-Cohen, S., Jolliffe, T., Mortimore, C., & Robertson, M. (1997). Another advanced test of theory of mind: Evidence from very high functioning adults with autism or asperger syndrome. Journal of Child Psychology and Psychiatry and Allied Disciplines, 38(7), 813-822.
- Freeth, M., Ropar, D., Mitchell, P., Chapman, P. & Loher, S. (2011). How adolescents with ASD process social information in complex scenes. Combining evidence from eye movements and verbal descriptions. Journal of autism and Developmental Disorders, 41, 364-371
- Frith, U. (2003). Autism, Explaining the Enigma, Second Edition. Oxford: Basil Blackwell.
- Klin, A., Jones, W., Schultz, R., Volkmar, F., & Cohen, D. (2002). Visual fixation patterns during viewing of naturalistic social situations as predictors of social competence in ndividuals with autism. Archives of General Psychiatry, 59(9), 809–816.
- Wing, L. & Gould, J. (1979). Severe impairments of social interaction and associated abnormalities in children: Epidemiology and classification. Journal of Autism and Developmental Disorders, 9, 11-29.
Header Image: Autism Awareness Ribbon (CC 3.0). Image can be viewed at http://commons.wikimedia.org/wiki/File:Autism_Awareness_Ribbon.png
No comments yet, fill out a comment to be the first






Leave a Reply